Aromatase inhibitors (AIs) are drugs that can lower estrogen in the body. They do this by inhibiting a specific enzyme. As you might have guessed, it's the enzyme called aromatase. Aromatase converts androgens into estrogen. For example, it converts the androgen testosterone to the estrogen estradiol.
There are currently three popular AIs in circulation, namely: exemestane (Aromasin), anastrozole (Arimidex) and letrozole (Femera). You'll see these drugs most commonly used in breast cancer treatment. A lot of research has therefore been performed in women. In women, AIs are very potent in lowering estrogen. For example, exemestane suppresses estradiol levels by 92% in postmenopausal breast cancer patients [1]. Similarly, letrozole and anastrozole suppresses estradiol levels by nearly 90%, also in postmenopausal breast cancer patients [2].
Aromatase inhibitors are less potent in men
Few trials have investigated the efficacy of aromatase inhibitors to lower estrogen in men. Their results differ from that found in women.
A trial in young men found that 25 mg exemestane suppressed estradiol by 62 %, 12 hours after intake [3]. After taking it daily for 10 days, a suppression of only 38 % was found 24 hours after the last administered dose. Notably, doubling the dosage to 50 mg daily did not lead to a larger decrease in estradiol levels.
Similar results are seen in young men receiving anastrozole for 10 days [4]. The administration of both 0.5 and 1 mg anastrozole daily lead to a decrease in estradiol levels of roughly 50 %. I'm unsure how relevant it is, but the authors did not mention how many hours after the last dose the measurements were taken.
Finally, letrozole is in the same ball park efficacy-wise as exemestane and anastrozole. After 28 days of letrozole treatment at 2.5 mg daily, estradiol was reduced by 46 % in young men and 62 % in elderly men [5]. It's unclear whether the difference between young men and elderly men is a real difference. The authors did not perform any statistical testing for it. In line with these results, another study found estradiol levels were reduced by 56 % in men receiving 2.5 mg letrozole daily for 4 weeks [6].
In sum, you could state that the three popular AIs are similarly effective in decreasing estrogen.
Aromatase inhibitors might be more potent when administering exogeneous testosterone
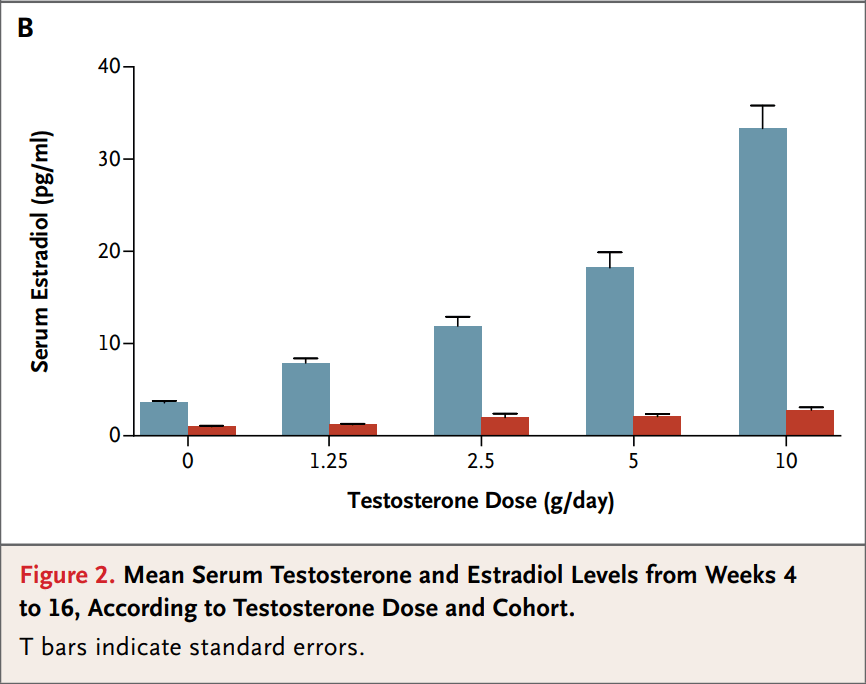
The above studies were undertaken in men producing their own (endogeneous) testosterone. But the situation appears to be different when endogeneous testosterone is replaced with exogeneous testosterone. Finkelstein et al. examined the effects of increasing amounts of testosterone with and without an aromatase inhibitors on a bunch of stuff [7]. A total of 198 healthy men were randomly allocated to placebo, 1.25, 2.5, 5, or 10 g of testosterone gel daily for 16 weeks, and another 202 also received the AI anastrozole in conjunction. (Endogenous production was suppressed by goserilin acetate injections.)
The picture below shows the effect on testosterone and estradiol levels. Note that the blue bars were the men receiving only testosterone and the red bars the ones receiving it in conjunction with anastrozole.
Why might aromatase inhibitors be more effective for decreasing estradiol in men receiving exogeneous testosterone?
Unfortunately, there is no direct research for this. But if I had to guess, I think it has to do with the conversion of testosterone to estradiol taking place in the testes. A substantial part of estradiol is produced by aromatase activity in the testes. Testosterone concentrations there are roughly 100 times higher than in circulation. Since AIs need to competitively inhibit aromatase, the dosages might need to be way higher in order to lead to sufficient inhibition of aromatase in the testes. But again, this is a guess from my side.
References
- J. Geisler, N. King, G. Anker, G. Ornati, E. Di Salle, P. Lønning, and M. Dowsett. In vivo inhibition of aromatization by exemestane, a novel irreversible aromatase inhibitor, in postmenopausal breast cancer patients. Clinical Cancer Research, 4(9):2089–2093, 1998.
- J. Geisler, B. Haynes, G. Anker, M. Dowsett, and P. Lonning. Influence of letrozole and anastrozole on total body aromatization and plasma estrogen levels in postmenopausal breast cancer patients evaluated in a randomized, cross-over study. Journal of Clinical Oncology, 20(3):751–757, 2002.
- N. Mauras, J. Lima, D. Patel, A. Rini, E. di Salle, A. Kwok, and B. Lippe. Pharmacokinetics and dose finding of a potent aromatase inhibitor, aromasin (exemestane), in young males. The Journal of Clinical Endocrinology & Metabolism, 88(12):5951–5956, 2003.
- N. Mauras, K. O. O’Brien, K. O. Klein, and V. Hayes. Estrogen suppression in males: metabolic effects. The Journal of Clinical Endocrinology & Metabolism, 85(7):2370–2377, 2000.
- G. G. T’sjoen, V. A. Giagulli, H. Delva, P. Crabbe, D. De Bacquer, and J.-M. Kaufman. Comparative assessment in young and elderly men of the gonadotropin response to aromatase inhibition. The Journal of Clinical Endocrinology & Metabolism, 90(10):5717–5722, 2005.
- G. Raven, F. H. de Jong, J.-M. Kaufman, and W. de Ronde. In men, peripheral estradiol levels directly reflect the action of estrogens at the hypothalamo-pituitary level to inhibit gonadotropin secretion. The Journal of Clinical Endocrinology & Metabolism, 91(9):3324–3328, 2006.
- J. S. Finkelstein, H. Lee, S.-A. M. Burnett-Bowie, J. C. Pallais, E. W. Yu, L. F. Borges, B. F. Jones, C. V. Barry, K. E. Wulczyn, B. J. Thomas, et al. Gonadal steroids and body composition, strength, and sexual function in men. New England Journal of Medicine, 369(11):1011–1022, 2013.